| Composition |
| Sacoplus 200: Each Film coated tablet contains: Sacubitril 97.2 mg +Valsartan 102.8 mg (as sacubitril valsartan sodium salt complex). |
| Contraindications |
• Hypersensitivity to the active substance or to any of the excipients.
• Concomitant use with ACE inhibitor, it must not be administrated until 36 hours after discounting ACE inhibitor therapy.
• Known history of angioedema related to previous ACE inhibitor or ARB therapy.
• Hereditary or idiopathic angioedema.
• Concomitant use with aliskiren – countaining medical products in patients with diabetes mellitus or in patients with renal impairment.
• Severe hepatic impairment, biliary cirrhosis and cholestasis.
• Second and third trimester of pregnancy.
|
| Indications |
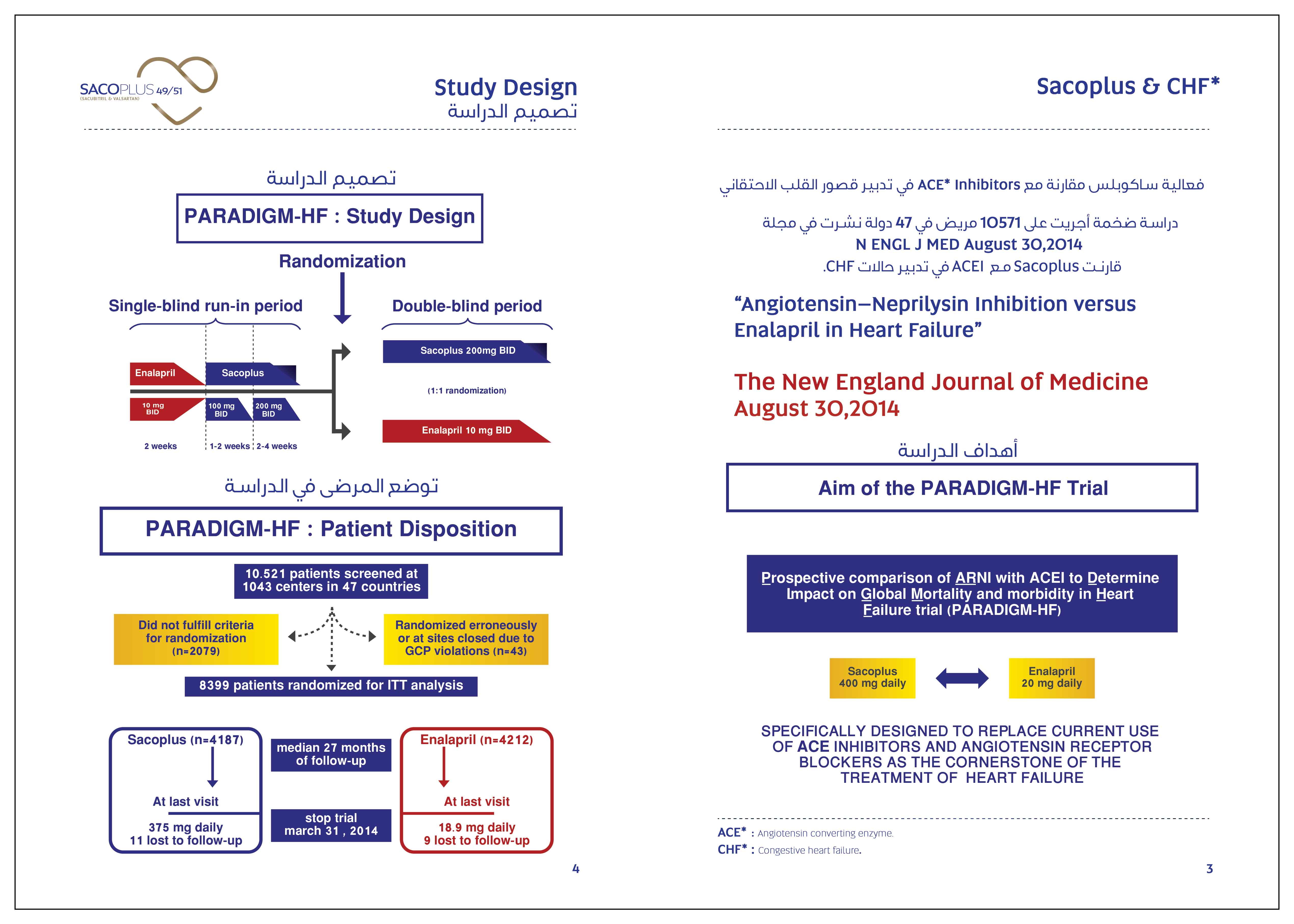
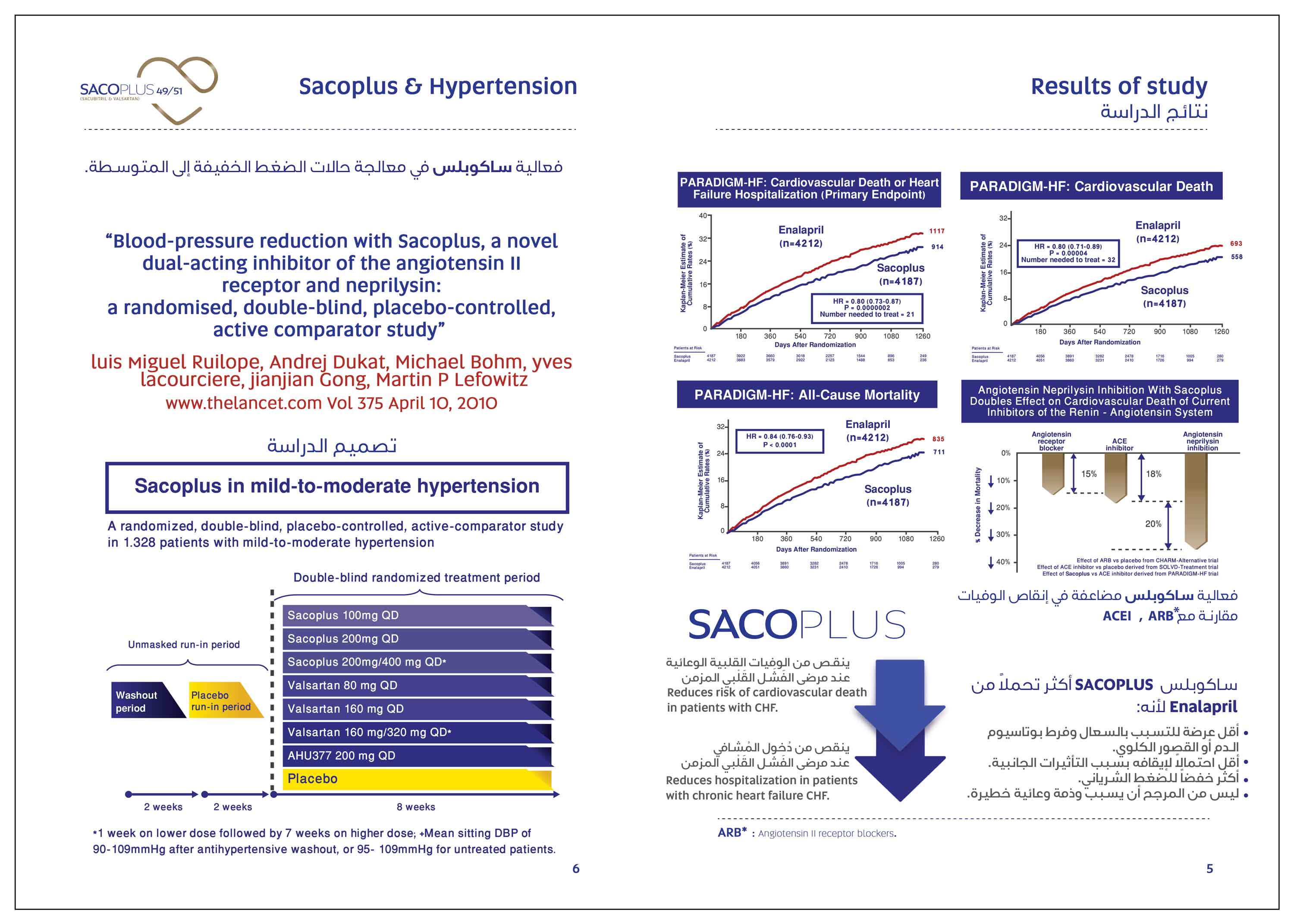
| It is indicated in adult patients for treatment of symptomatic chronic heart failure with reduced ejection fraction and it reduce the risk of cardiovascular death and hospitalaization for heart failure patients with chronic heart failure (NYHA Class II-IV) and reduced ejection fraction. |
| Warnings and precautions |
Hypotension: Treatment should not be initiated unless SBP is ≥100 mmHg. Cases of symptomatic hypotension have been reported in patients treated with this drug especially in paitents ≥ 65 years old, Patients with renal disease and Patients with low SBP < 112 mmHg. When initiating therapy or during dose titration, blood pressure should be monitored routinely. If hypotension occurs, temporary down-titration or discontinuation of the therapy is recommended. Symptomatic hypotension is more likely to occur if the patient has been volume depleted e.g. by diuretic therapy, dietary salt restriction, diarrhea or vomiting. Sodium and/or volume depletion should be corrected before starting treatment. However, such corrective action must be carefully weighed against the risk of volume overload.
Impaired renal function: Evaluation of patients with heart failure should always include assessment of renal function. Patients with mild and moderate renal impairment are more at risk of developing hypotension. There is no experience in patients with end-stage renal disease and use of this drug is not recommended.
Worsening renal function: Use of this drug may be associated with decreased renal function. The risk may be further increased by dehydration or concomitant use of non-steroidal anti-inflammatory agents (NSAIDs). Down-titration should be considered in patients who develop a clinically significant decrease in renal function.
Hyperkalaemia: Treatment should not be initiated if the serum potassium level is > 5,4 mmol/l. the use of this drug may be associated with an increased risk of hyperkalaemia. Monitoring of serum potassium is recommended, especially in patients who have risk factors such as renal impairment, diabetes mellitus or hypoaldosteronism or who are on a high potassium diet or on mineralocorticoid antagonists. If serum potassium level is >5.4 mmol/l discontinuation should be considered.
Angioedema: Angioedema has been reported in patients treated with this drug. If angioedema occurs, it should be immediately discontinued and appropriate therapy and monitoring should be provided until complete resolution of signs and symptoms has occurred. It must not be re-administered .Angioedema associated with laryngeal oedema may be fatal. Where there is involvement of the tongue, glottis or larynx likely to cause airway obstruction, appropriate therapy should be promptly administered.
Patients with a prior history of angioedema were not studied. As they may be at higher risk for angioedema, caution is recommended if this drug is used in these patients.
This drug is contraindicated in patients with a known history of angioedema related to previous ACE inhibitor or ARB therapy or with hereditary or idiopathic angioedema. Black patients have an increased susceptibility to develop angioedema.
Patients with renal artery stenosis: this drug may increase blood urea and serum creatinine levels in patients with bilateral or unilateral renal artery stenosis. Caution is required in patients with renal artery stenosis and monitoring of renal function is recommended.
B-type natriuretic peptide (BNP): BNP is not a suitable biomarker of heart failure in patients treated with this drug because it is a neprilysin substrate.
|
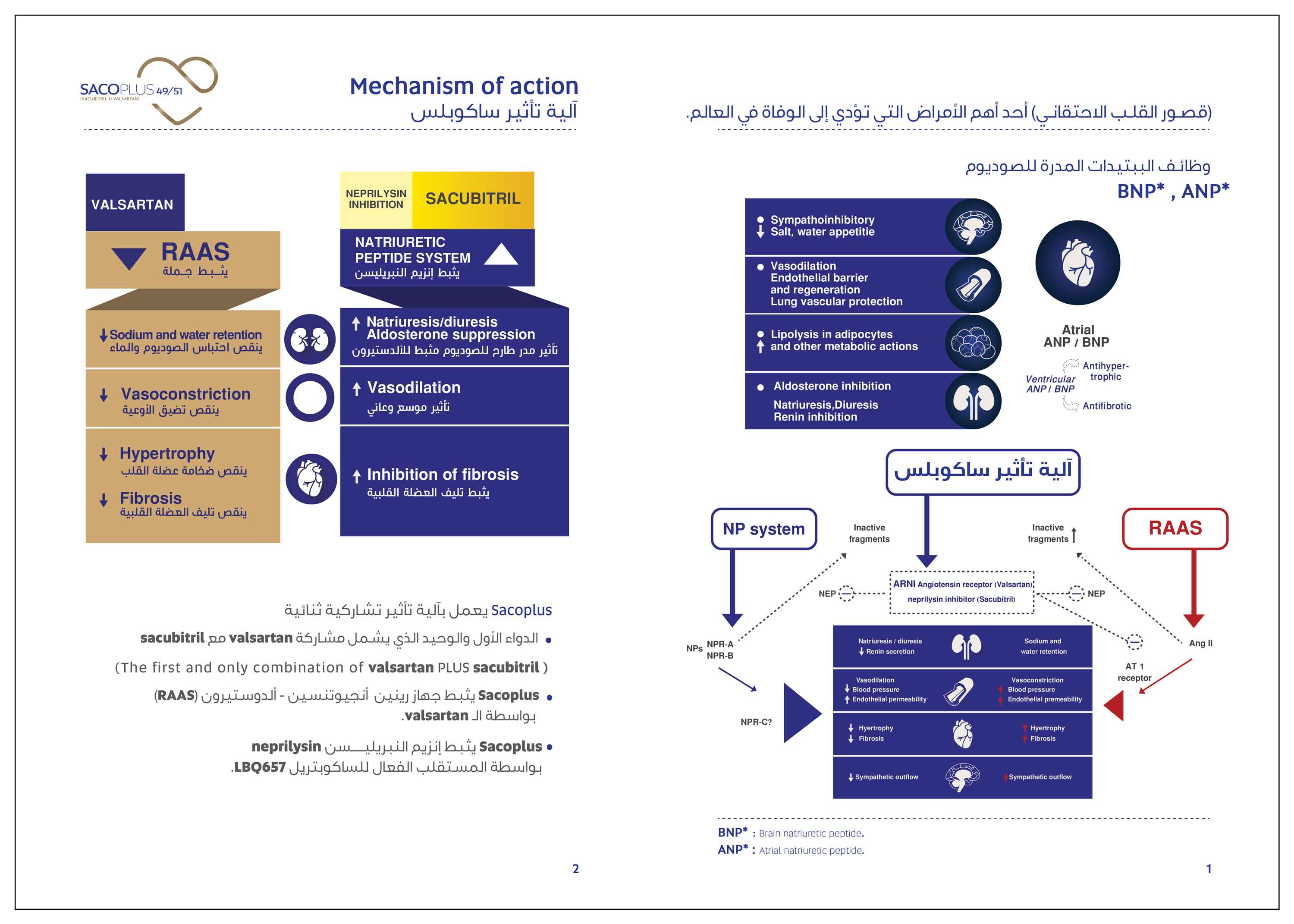
| Mechanism of action |
| This product exhibits the mechanism of action by simultaneously inhibiting neprilysin ( neutral endopeptidase: NEP ) via LBQ657. The active metabolite of the prodrug sacubitril, and by blocking the angiotensin Π type-1 (AT1) receptor via valsartan which is also inhibits angiotensin II – dependent aldosterone release. |
| Pharmacokinetic properties |
Absorption: Following oral administration, the drug dissociates into valsartan and the prodrug sacubitril. Sacubitril is further metabolised to the active metabolite LBQ657. These reach peak plasma concentrations in 2 hours, 1 hour, and 2 hours, respectively. The oral absolute bioavailability of sacubitril and valsartan is estimated to be more than 60% and 23%, respectively.
Administration with food has no clinically significant impact on the systemic exposures of sacubitril, LBQ657 and valsartan. This drug can be administered with or without food.
Distribution: Sacubitril, LBQ657 and valsartan are highly bound to plasma proteins (94-97%). LBQ657 crosses the blood brain barrier to a limited extent (0.28%).
Biotransformation: Sacubitril is readily converted to LBQ657; LBQ657 is not further metabolised to a significant extent. Valsartan is minimally metabolised, as only about 20% of the dose is recovered as metabolites.
Since CYP450-enzyme-mediated metabolism of sacubitril and valsartan is minimal, co-administration with medicinal products that impact CYP450 enzymes is not expected to impact the pharmacokinetics.
Elimination: Following oral administration, 52-68% of sacubitril (primarily as LBQ657) and ~13% of valsartan and its metabolites are excreted in urine; 37-48% of sacubitril (primarily as LBQ657) and 86% of valsartan and its metabolites are excreted in faeces.
Sacubitril, LBQ657 and valsartan are eliminated from plasma with a mean elimination half-life (T½) of approximately 1.43 hours, 11.48 hours, and 9.90 hours, respectively.
|
| Excipients |
Hydroxypropylcellulose, Microcrystalline cellulose, Crospovidone, Magnesium stearate
Talc, Aerosil ,. Hypromellose, Titanium dioxide, Macrogol 4000, Talc, Colore (Iron oxide red, Brilliant Blue E133).
|
| Drug Interaction |
1. Interactions that is contraindicated:
ACE inhibitors: The concomitant use with ACE inhibitors is contraindicated and may increase the risk of angioedema. It must not be started until 36 hours after taking the last dose of ACE inhibitor therapy. ACE inhibitor therapy must not be started until 36 hours after the last dose of this drug.
Aliskiren: The concomitant use with aliskiren-containing products is contraindicated in patients with diabetes mellitus or in patients with renal impairment (eGFR <60 ml/min/1.73 m2). The combination of this drug with direct renin inhibitors such as aliskiren is not recommended. The combination with aliskiren is potentially associated with a higher frequency of adverse events such as hypotension, hyperkalemia and decreased renal function (including acute renal failure).
2. Interactions requiring in concomitant use not being recommended: This drug contains valsartan and therefore it should not be co-administered with another ARB or ACE inhibitors containing product.
3. Interactions requiring precautions:
OATP1B1 (Organic Anion Transporting Polypeptide 1B1) and OATP1B3 substrates, e.g. statins: this drug may increase the systemic exposure of OATP1B1 and OATP1B3 substrates such as statins. Caution should be exercised when co-administering this drug with statins.
PDE5 inhibitors including sildenafil: Addition of a single dose of sildenafil to this drug at steady state in patients with hypertension was associated with a significantly greater blood pressure reduction compared to administration of it alone. Therefore Caution should be exercised when sildenafil or another PDE5 inhibitor is initiated in patients treated with this drug.
Potassium: Concomitant use with potassium-sparing diuretics (triamterene, amiloride), mineralocorticoid antagonists (e.g. spironolactone, eplerenone), potassium supplements and salt substitutes containing potassium or other agents (such as heparin) may lead to increases in serum potassium, and to increase in serum creatinine. Monitoring of serum potassium is recommended if this drug is co-administered with these agents.
OATP and MRP2 (multi drug resistant protein) transporters: The active metabolite of sacubitril (LBQ657) and valsartan are OATP1B1, OATP1B3, OAT1 and OAT3 substrates; valsartan is also a MRP2 substrate. Therefore, co-administration of this drug with inhibitors of OATP1B1, OATP1B3, OAT3 (e.g. rifampicin, ciclosporin), OAT1 (e.g. tenofovir, cidofovir) or MRP2 (e.g. ritonavir) may increase the systemic exposure of LBQ657 or valsartan. Appropriate care should be exercised when initiating or ending concomitant treatment with such medicinal products.
Furosemide: Co-administration of this drug and furosemide had no effect on the pharmacokinetics of this drug but reduced Cmax and AUC of furosemide by 50% and 28%, respectively.
Non-steroidal anti-inflammatory agents (NSAIDs), including (COX-2) inhibitors: In elderly patients, volume-depleted patients (including those on diuretic therapy), or patients with compromised renal function, the concomitant use of this drug and NSAIDs may lead to an increased risk of worsening of renal function. Therefore, monitoring of renal function is recommended when initiating or modifying treatment in patients on this drug who are taking NSAIDs concomitantly.
Lithium: Reversible increases in serum lithium concentrations and toxicity have been reported during concomitant administration of lithium with ACE inhibitors or angiotensin II receptor antagonists. Therefore, this combination is not recommended. If a diuretic is also used, the risk of lithium toxicity may be increased further.
Metformin: Co-administration with metformin reduced both Cmax and AUC of metformin by 23%. When initiating therapy with this drug in patients receiving metformin, the clinical status of the patient should be evaluated.
|
| Pregnancy and lactation |
Pregnancy: The use of this drug is not recommended during the first trimester of pregnancy and is contraindicated during the second and third trimesters of pregnancy.
If exposure to ARBs has occurred from the second trimester of pregnancy, ultrasound check of renal function and skull is recommended. Infants whose mothers have taken ARBs should be closely observed for hypotension.
There are no data from the use of this drug in pregnant women. Animal studies with this drug have shown reproductive toxicity.
Breast-feeding: It is not known whether this drug is excreted in human milk. Because of the potential risk in breast-fed/newborns, it is not recommended during breast-feeding. A decision should be made whether to abstain from breast-feeding or to discontinue the drug while breast-feeding, taking into account the importance of the drug to the mother.
|
| Effects on ability to drive and use machines |
| It has a minor influence on the ability to drive and use machines. When driving vehicles or operating machines it should be taken into account that occasionally dizziness or fatigue may occur. |
| Undesirable effects |
Very common adverse reactions: hyperkalaemia, hypotension and renal impairment.
Common adverse reactions: Anemia, Hypoglycemia, hypokalemia, dizziness, Headache, Syncope, vertigo, orthostatic hypotension, Cough, diarrhoea, Nausea, Gastritis, Fatigue, Asthenia, Renal failure.
Uncommon Undesirable effect: Hypersensitivity, postural Dizziness, Pruritus, Rash, Angioedema.
|
| DOSAGE & ADMINISTRATION |
It may be administrated with or without food. The tablets must be swallowed with a glass of water
• The recommended starting dose is one tablet of 49/51 mg twice-daily, except in the situations described below
• The dose should be doubled at 2-4 weeks to the target dose of one tablet of 97/103 mg twice-daily, as tolerated by the patient
• If Patients experience tolerability issue (systolic blood pressure [SBP] ≤ 95mmHg, symptomatic hypotension, hyperkalemia, renal dysfunction), adjustment of concomitant medicinal product, temporary down-titration or discontinuation of the drug is recommended.
• There is limited experience in patients not currently taking an ACE inhibitor or an ARB or taking low doses of these medicinal products, therefore a Starting dose of 24 mg/26mg twice daily and slow dose titration ( doubling every 3-4 weeks ) are recommended in these patients.
• Treatment should not be initated in patients with serum potassium level > 5,4 mmol/l or with SBP < 100 mmHg. A starting dose of 24 mg / 26 mg twice daily should be considered for patients with SBP≥ 100 to 110 mmHg.
• If a dose is missed, the patient should take the next dose at the scheduled time.
Use in Elderly patients: The dose should be in line with the renal function of the elderly patient.
Renal impairment:
Mild renal impairment (eGFR 60 – 90 ml/min/1,73m2): No dose adjustment is required.
Moderate renal impairment (eGFR 30-60 ml/min/1,73m2): A starting dose of 24 mg/ 26 twice daily should be considered
Severe renal impairment (eGFR <30 ml/min/1,73m2): it should be used with caution and a starting dose of 24 mg/26 mg twice daily is recommended.
End stage renal disease: it is not recommended.
Hepatic impairment: there is limited experience in patients with moderate hepatic impairment) or with AST/ALT values more than twice the upper limit of the normal range: it should be used with caution in these patients, and the recommended starting dose 24 mg /26 mg twice daily.
It is contraindicated in patients with severe hepatic impairment, biliary cirrhosis or cholestasis.
Use in Pediatric patients: The safety and efficacy of this drug in Children and adolescents aged below 18 years have not been established.
|
| Overdose |
| Hypotension is the most likely symptom of overdose due to the blood pressure lowering effects of this drug, Symptomatic treatment should be provided. This product is unlikely to be removed by haemodialysis due to high protein binding. |
| Packaging |
Sacoplus 200: Pack contains 20 film coated tablets. |