| Composition |
amlodipine besylate and benazepril hydrochloride Combination Capsules
2.5 mg/10 mg
5 mg/10 mg
5 mg/20 mg
10 mg/20 mg |
| Pharmaceutical Category |
| Drug is a combination of amlodipine besylate and benazepril hydrochloride. |
| Pharmacodynamics properties |
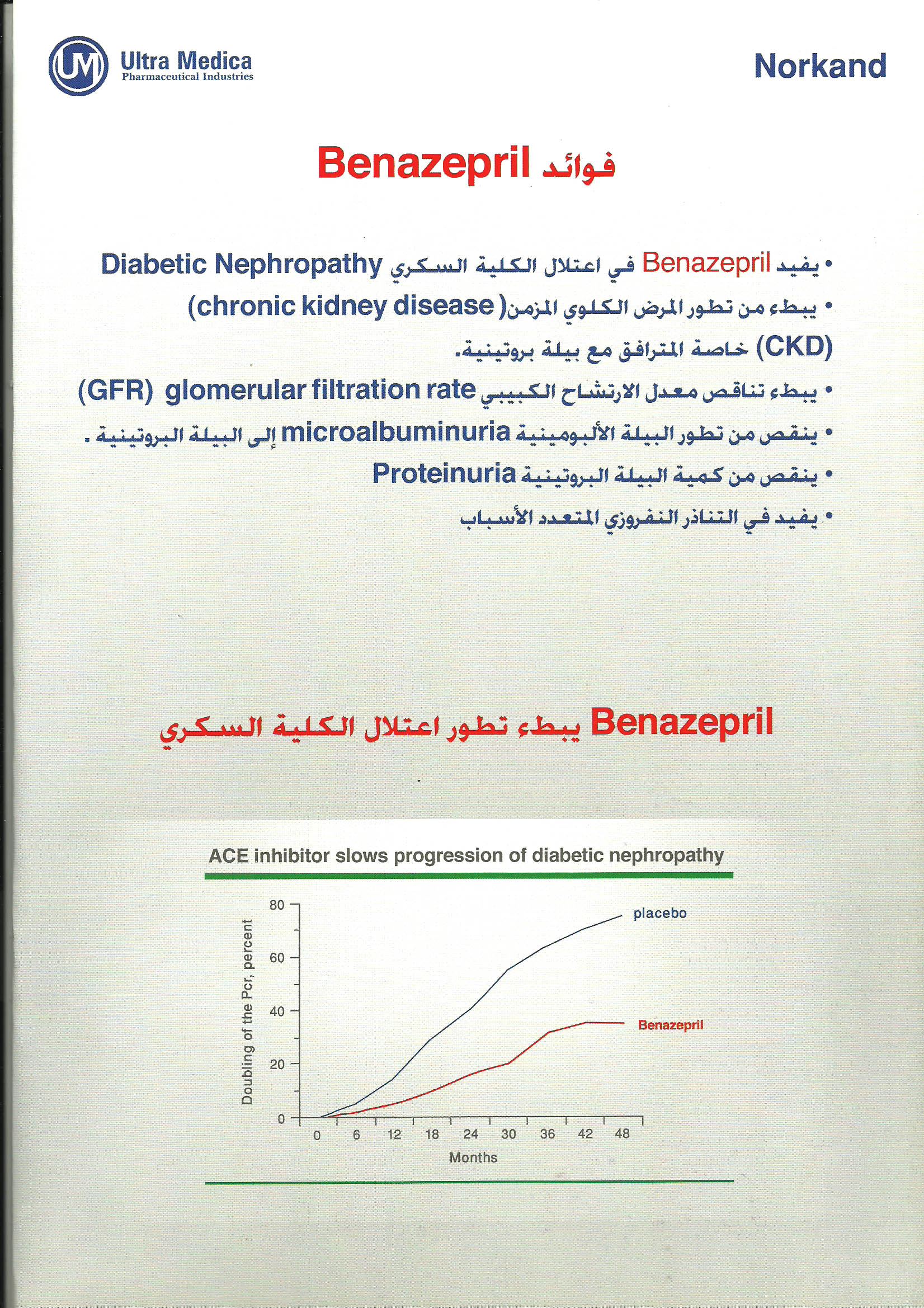
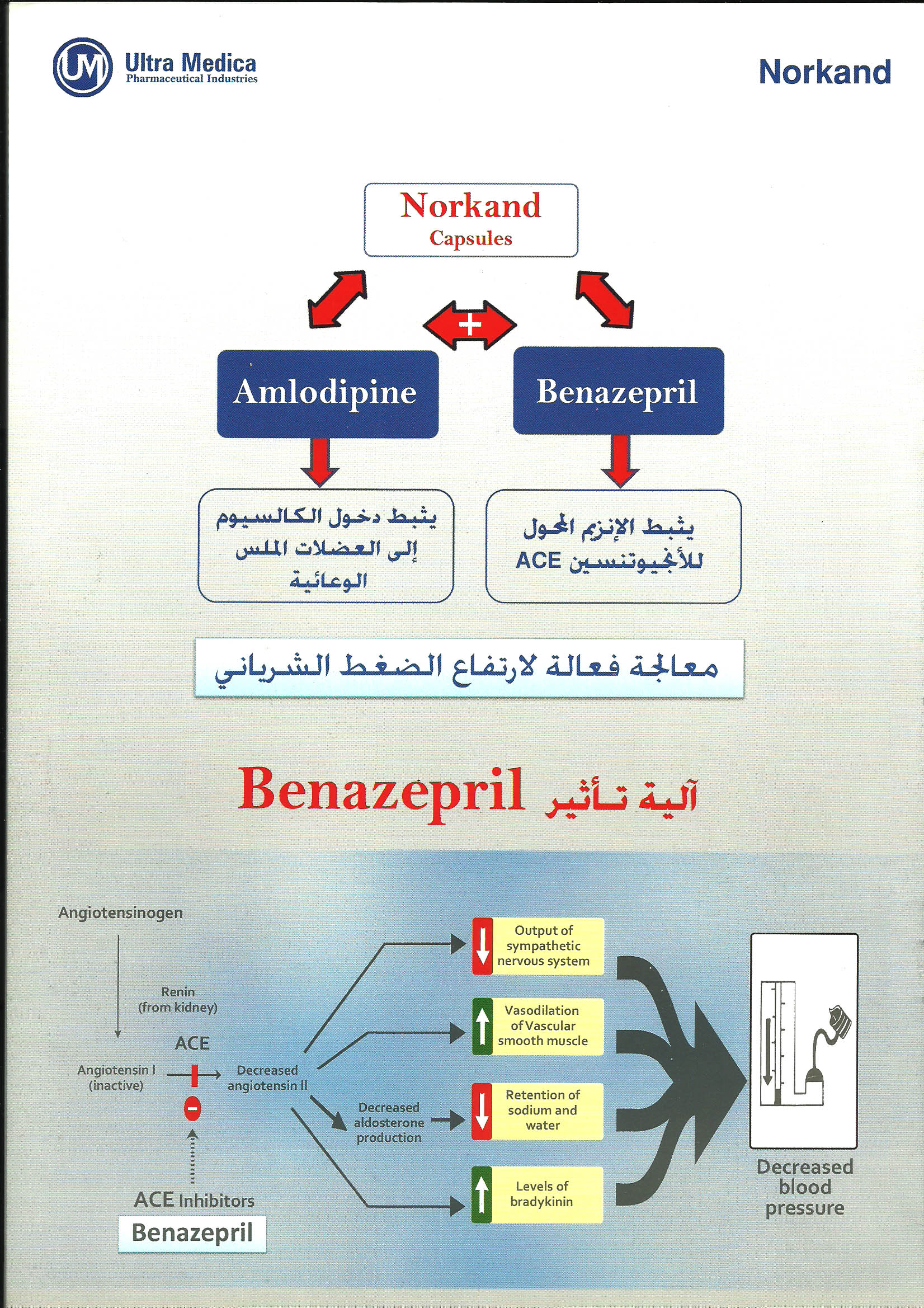
Benazepril and benazeprilat inhibit angiotensin-converting enzyme (ACE). ACE is a peptidyl dipeptidase that catalyzes the conversion of angiotensin I to the vasoconstrictor substance angiotensin II. Angiotensin II also stimulates aldosterone secretion by the adrenal cortex. Inhibition of ACE results in decreased plasma angiotensin II, which leads to decreased vasopressor activity and to decreased aldosterone secretion. The latter decrease may result in a small increase of serum potassium.
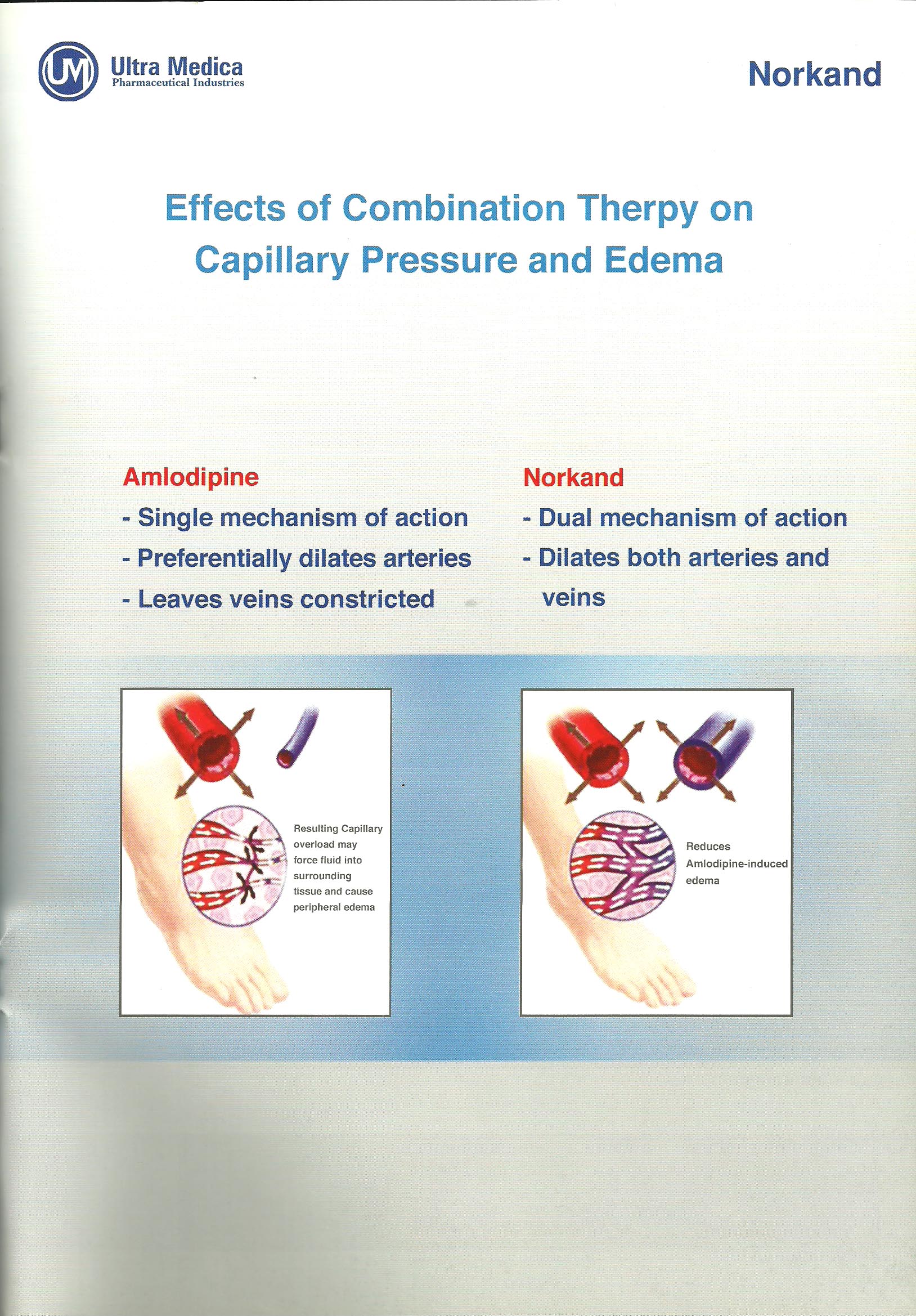
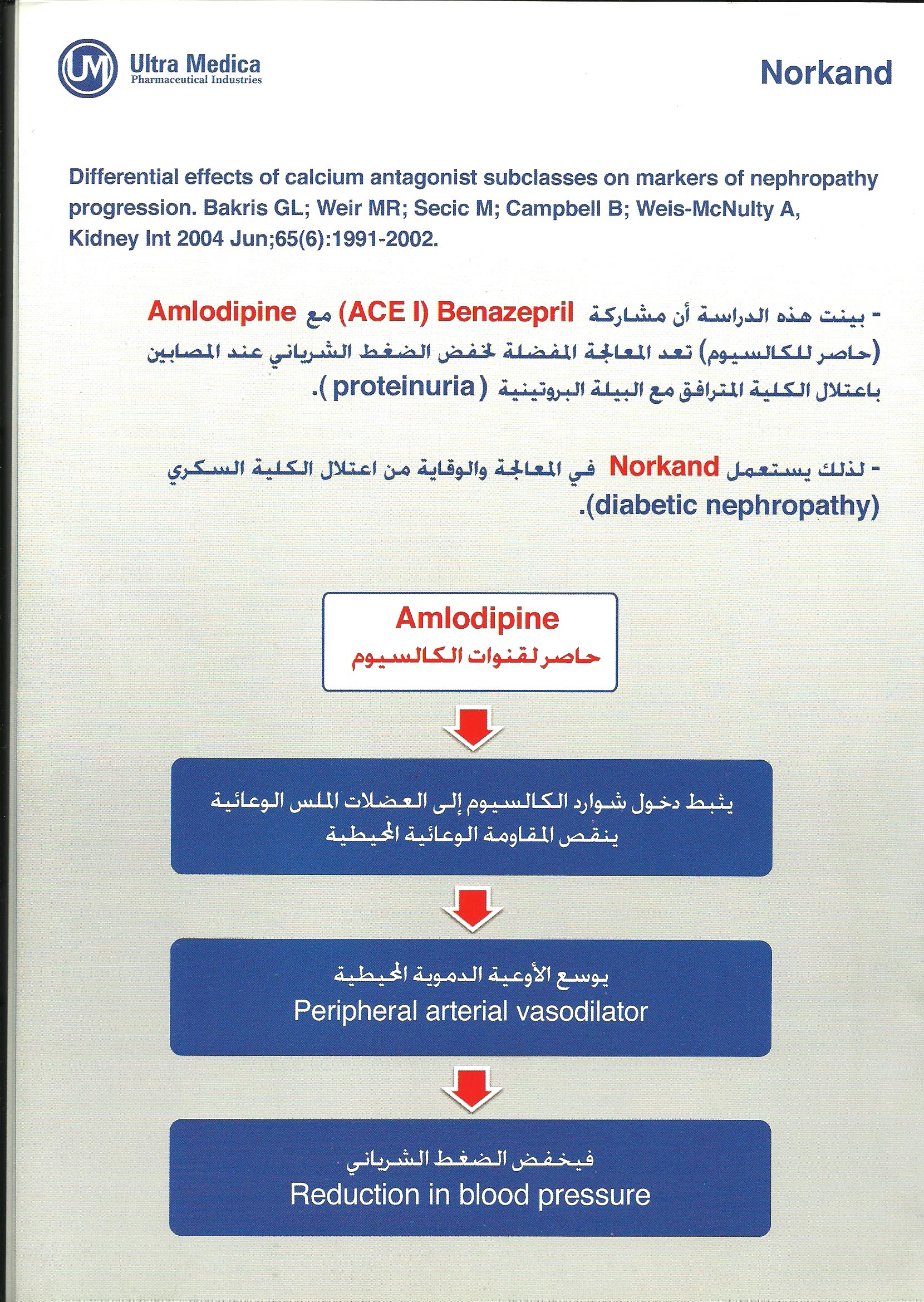
Amlodipine is a dihydropyridine calcium antagonist that inhibits the transmembrane influx of calcium ions into vascular smooth muscle and cardiac muscle. Serum calcium concentration is not affected by amlodipine. Amlodipine is a peripheral arterial vasodilator that acts directly on vascular smooth muscle to cause a reduction in peripheral vascular resistance and reduction in blood pressure. |
| Pharmacokinetics |
Absorption from the individual tablets is not influenced by the presence of food in the gastrointestinal tract. Following oral administration of this drug, peak plasma concentrations of benazepril are reached in 0.5-2 hours. Cleavage of the ester group (primarily in the liver) converts benazepril to its active metabolite, benazeprilat. Peak plasma concentrations of amlodipine are reached 6-12 hours after administration of Drug. Only trace amounts of an administered dose of benazepril can be recovered unchanged in the urine.
Amlodipine is extensively metabolized in the liver, with 10% of the parent compound and 60% of the metabolites excreted in the urine. In patients with hepatic dysfunction, decreased clearance of amlodipine may increase the area-under-the-plasma-concentration curve, and dosage reduction may be required. In patients with renal impairment, the pharmacokinetics of amlodipine are essentially unaffected. Benazeprilat's effective elimination half-life is 10-11 hours, while that of amlodipine is about 2 days, so steady-state levels of the two components are achieved after about a week of once-daily dosing. |
| Therapeutic indications |
Drug is indicated for the treatment of hypertension.
This drug is not indicated for the initial therapy of hypertension |
| Side effect |
| it may be happend in some cased angioedema , fatigue , insomnia , nervousness , anxiety , tremor , flushing , rash , nausea , dry mouth , abdominal hyperkalemia , back pain and muscle cramps. |
| Warnings and precautions |
Warnings
Angioedema of the face, extremities, lips, tongue, glottis, and larynx has been reported in patients treated with ACE inhibitors. If laryngeal stridor or angioedema of the face, tongue, or glottis occurs. This drug can cause symptomatic hypotension. Rarely, ACE inhibitors have been associated with a syndrome that starts with cholestatic jaundice and progresses to hepatic necrosis. Patients receiving ACE inhibitors who develop jaundice or marked elevations of hepatic enzymes should discontinue the ACE inhibitor and receive appropriate medical follow-up.
Precautions
Drug should be used with caution in patients with severe renal disease, hyperkalemia, heart failure, hepatic dysfunction. Presumably due to the inhibition of the degradation of endogenous bradykinin, persistent nonproductive cough has been reported with all ACE inhibitors, always resolving after discontinuation of therapy. |
| Contraindication |
| Drug is contraindicated in patients who are hypersensitive to benazepril, to any other ACE inhibitor, or to amlodipine. |
| Pregnancy and lactation |
USE IN PREGNANCY
When used in pregnancy during the second and third trimesters, ACE inhibitors can cause injury and even death to the developing fetus. When pregnancy is detected, drug should be discontinued as soon as possible.
Nursing Mothers
Minimal amounts of unchanged benazepril and of benazeprilat are excreted into the breast milk of lactating women treated with benazepril.
It is not known whether amlodipine is excreted in human milk. In the absence of this information, it is recommended that nursing be discontinued while drug is administered. |
| Drug interactions |
Potassium Supplements and Potassium-Sparing Diuretics: Benazepril can attenuate potassium loss caused by thiazide diuretics. Potassium-sparing diuretics (spironolactone, amiloride, triamterene, and others) or potassium supplements can increase the risk of hyperkalemia.
Lithium Increased serum lithium levels have been reported in patients receiving ACE inhibitors during therapy with lithium. |
| DOSAGE & ADMINISTRATION |
Amlodipine is an effective treatment of hypertension in once-daily doses of 2.5-10 mg while benazepril is effective in doses of 10-80 mg. Dosage must be guided by clinical response.
This drug is not indicated for the initial therapy of hypertension.
Use in Patients With Metabolic Impairments: Regimens of therapy with this drug need not
take account of renal function as long as the patient’s creatinine clearance is
>30 mL/min/1.73m2 (serum creatinine roughly ≤3 mg/dL or 265 μmol/L). In patients with
more severe renal impairment, the recommended initial dose of benazepril is 5 mg. This drug is
not recommended in these patients. |