| Composition |
Londalop is an inhibitor of HMG-CoA reductase.
It is a synthetic lipid-lowering agent for oral administration.
Each F.C tablet of Londalop1 contains 1.045mg of pitavastatin which is equivalent to 1mg of free base.
Each F.C tablet of Londalop2 contains 2.09 mg of pitavastatin which is equivalent to 2 mg of free base.
Each F.C tablet of Londalop4 contains 4.18 mg of pitavastatin which is equivalent to 4 mg of free base. |
| Pharmacodynamics properties |
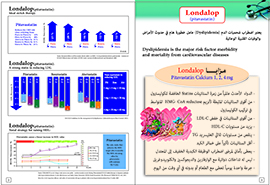
LONDALOP competitively inhibils HMG-CoA reductase, which is an enzyme involved with biosynthesis of cholesterol, in a manner of competition with the substrate so that it inhibit cholesterol synthesis in the liver. As a result, the expression of LDL-receptors followed by the uptake of LDL from blood to liver is accelerated and then the plasma TC decreases.
Further, the sustained inhibition of coolesterol synthesis in the liver decreases levels of very low density lipoproteins. |
| Pharmacokinetics |
Absorption: Pitavastatin peak plasma concentrations are achieved about 1 hour after oral administration. The absolute bioavailabilify of pitavastatin oral solution is 51%. Administration of LONDALOP with a high fat meal (50% fat contentl decreases pitavastatin Cmax but does not significantly reduce pitavastatin AUC. The Cmax and AUC of pitavastatin did not differ following evening or morning drug administration.
Distribution: LONDALOP is more than 99f, protein bound in human plasma, mainly to albumin & alpha 1-acid glycoprotein, and the mean volume of distribution is approximately 148 L.
Metabolism : LONDALOP is marginally metabolized by CYP2C9 and to a lesser extent by CYP2CB. The major metaboltte in human plasma is the lactone which is formed via an ester-type pitavastatin glucuronide conjugate.
Excretion: A mean of 15r. of orally administered single 32 mg pitavastatin dose was excreted in urine, whereas a mean of 79% of the dose was excreted in feces witl'in 7 days. The mean plasma elimination ha"-I~e is approximately 12 hours. |
| Therapeutic indications |
INDICATIONS : Drug therapy s~ould be one component of multiple-risk-factor intervention in individuals who require modifications of their lipid profile.
Lipid-altering agents should be used in addition to a diet restricted in saturated fat and cholesterol only when the response to diet and other non pharmacological measures has been inadequate.
1.1. Primary Hyperlipidemia and Mixed Dyslipidemia LONDALOP is indicated as an adjunctive therapy to diet to reduce elevated total coolesterol (TC), low-density lipoprotein coolesteroIILDL-C), apolipoprotein B (Apo B), triglycerides (TG), and to increase HDL-C in adult patients with primary hyperlipidemia or mixed dyslipidemia.
LIMITATIONS OF USE : Doses of Londalop greater than 4 mg once daily were associated with an increased risk for myopathy in premarketing clinical studies.
Do not exceed 4 mg once daily dosing of Londalop.
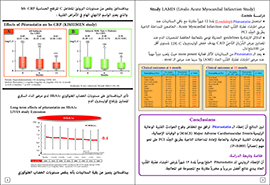
The eHect of Londalop on cardiovascular morbidity and mortality has not been determined.
Londalop has not been studied in patients with severe renal impairment (glomerular filtration rate < 30 mLiminl1 .73 m2) not on hemodialysis.
Londalop should not be used in this patient population.
Londalop has not been studied with the protease inhibitor combination lopinavir/ritonavir. Londalop should not be used with tl'is combination of protease inhibitors.
Londalop has not been studied in Fredrickson Type I, III, and V dyslipidemias. |
| Side effect |
The following serious adverse effects may occur when adminls1tated the drug :
• Rhabdomyolysis with myoglobinuria and renal failure and (including myosttis).
• Uver Enzyme Abnormalities. Elevated creatine phospookinase (which is the most common reactiOn), transaminases. alkaline pt-csphate, bilirubin, and glucose.
• Other adverse reactions reported from clinical studies were arthralgia . headache, influenza, and nasopharyngitis.
• Back Pain, Constipation, Diarrhea, Myalgia I Pain in extremity , |
| Warnings and precautions |
Skeletal Muscle Effects: Cases of myopathy and rhabdomyolysis with renal failure secondary to myoglobinuria have been reporfed with HMG-CoA reductase inhibitors, including Londalop.
The eHect of Londalop on cardiovascular morbid tty and mortality has not been determined.
These risks can occur at any dose leVel. but increase in a dose-dependent manner.
Tl'is drug soould be prescribed with caution in patients with predisposing factors for myopathy. These factors include advanced age> 65 years, renal impairment, and inadequately treated hypothyroidism.
The risk of myopathy may also be increased with concurrent administration of fibrates or lipid-modifying doses of niacin.
Londalop therapy should be discontinued if markedly elevated creatine kinase (CK) levels occur or myopathy is diagnosed or suspected.
Londalop therapy should also be temporarily withheld in any patienl with an acute, serious condttion suggestive of myopathy or predisposing to the developmenl of renal failure secondary to rhabdomyolysis (e.g., sepsis, hypotension, dehydration, major surgery, trauma, severe metabolic, endocrine, and electrolyte disorders, or uncontrolled seizures).
Palients should be advised to promptly report unexplained muscle pain, or weakness, particularly ij accompanied by malaise or fever.
Liver Enzyme Abnormalities and Monitoring: Increases in serum transaminases have been reported wtth HMG-CoA reductase inhibitors.
In most cases, the elevations were transient and resolved or improved on continued fherapy or after a brief interruption in therapy.
If is recommended that liver enzyme tests be performed belore and at 12 weeks following both the inttlation of therapy and any elevation of dose and periodically thereafter.
Patients who develop increased transaminase levels should be monitored until the abnormalities have resolved.
Should an increase in AL T or AST of >3 times upper limtt of normal persist, reduction of dose or withdrawal of drug is recommended. |
| Contraindication |
The use of LONDALOP Is contraindicated In the following conditions :
• Patients with a known hypersensitivity to any component of this product. Hypersensitivity reactions including rash, pruritus, and urticaria have been reported with LONDALOP .
• Patients with active liver disease which may include unexplained persistent elevations of hepatic transaminase levels.
• Women who are pregnant or may become pregnant. Because HMG-CoA reductase inhibttors decrease coolesferol synthesis and possibly the synthesis of other biologically active substances derived from cholesterol, LONDALOP may cause fetal harm when administered to pregnant women. If the patient becomes pregnant while taking this drug, the patient should be apprisd of the potential hazard to the fetus.
• Nursing mothers. Animal studies have shown that LONDALOP passes into breast milk. Since HMG-CoA reductase inhibitors have the potential to cause adverse reactions in nursing infants, pitavastatin, like other HMG-CoA reductase inhibitors, is contraindicated in pregnant or nursing mothers.
• Co-administration with cyclosporine. |
| Pregnancy and lactation |
Pregnancy
Pregnancy Category X, LONDALOP is contraindicated in women who are or may become pregnant.
There are no adequate and well-controlled studies of LONDALOP in pregnant women. LONDALOP may cause fetal harm when administered to a pregnanf woman.
If the patient becomes pregnant while taking LONDALOP, the patient should be apprised of the potential risks to the fetus and the lack of known clinical benefit wilh continued use during pregnancy.
Nursing Mothers
It is not known whether LONDALOP is excreted in human milk. Women who require pitavastatin treatment should be advised not 10 nurse their infants or to discontinue LONDALOP.
PEDIATRIC USE
Safety and eHectiveness of LONDALOP in pediatric patients have not been established. |
| Drug interactions |
• Cyclosporine: Cyclosporine significantly increased LONDALOP exposure. Co-administration of cyclosporine with LONDALOP is contraindicated.
• Lopinavir/Rltonavir : Lopinavir/ritonavir. with LONDALOP may significantly increase LONDALOP exposure. Therefore, LONDALOP should not be used with this combination of protease inhibitors. .•
Erythromycin: Erythromycin significantly increased LONDALOP~..:r, ' (.L\ In patients taking erythromycin, a dose of LONDALOP 1 mg once daily should not be exceeded.
• Rijampin : Rifampin significantly increased LONDALOP exposure. In patients taking rijampin, a dose of LONDALOP 2 mg once daily should not be exceeded.
• Fibrates : Because it is known that the risk of myopathy during treatment with HMG-CoA reductase inhibitors may be increased with concurrent administration of fibrates, LONDALOP should be administered with caution when used concomitantly with gemfibrozil or other.
• Niacin : The risk of skeletal muscle effects may be enhanced when LONDALOP is used In combination with niacin; a reduction in LONDALOP dosage should be considered in this setting.
• Warfarin: LONDALOP had no significant pharmacokinetic interaction w.a!l R-and S-warfarin. LONDALOP had no significant effect on prothrombin ~ (PT) and international normalized ratio when administered to patients receiving chronic warfarin treatment. |
| DOSAGE & ADMINISTRATION |
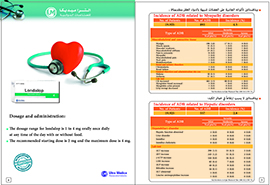
General Dosing Infonmation : The dose range for LONDALOP is 1 to 4 mg orally once daily at any time of the day with or without food.
The recommended stSJti1l9' dose is 2 mg and the maximum dose is 4 mg. The starting dose and maintenance doses of LONDALOP should be individualized according to patient characteristics.
such as goal of therapy and response.
After inttiation or upon tttration of LONDALOP, lipid levels should be analyzed after 4 weeks and the dosage adjusted accordingly.
Dosage in Patients with Renal Impairment : Patients wtth moderate renal impairmenl (glomerular filtration rate 30 to < 60 mL/mln/m21 and end -stage renal disease receiving hemodialysis should receive a starting dose of LONDALOP 1 mg once daily and a maximum dose of LONDALOP 2 mg once daily.
LONDALOP should not be used in patients with severe renal impairment (glomerular liltration rate < 30 mLimin/l .73 m2) not yet on hemodialysis.
Use with Erythromycin : In patients taking erythromycin, a dose of LONDALOP 1 mg once daily should not be exceeded.
Use with Rifampin : In patients taking rifampin, a dose of LONDALOP 2 mg once daily should not be exceededGeneral Dosing Infonmation : The dose range for LONDALOP is 1 to 4 mg orally once daily at any time of the day with or without food.
The recommended stSJti1l9' dose is 2 mg and the maximum dose is 4 mg. The starting dose and maintenance doses of LONDALOP should be individualized according to patient characteristics.
such as goal of therapy and response.
After inttiation or upon tttration of LONDALOP, lipid levels should be analyzed after 4 weeks and the dosage adjusted accordingly.
Dosage in Patients with Renal Impairment : Patients wtth moderate renal impairmenl (glomerular filtration rate 30 to < 60 mL/mln/m21 and end -stage renal disease receiving hemodialysis should receive a starting dose of LONDALOP 1 mg once daily and a maximum dose of LONDALOP 2 mg once daily.
LONDALOP should not be used in patients with severe renal impairment (glomerular liltration rate < 30 mLimin/l .73 m2) not yet on hemodialysis.
Use with Erythromycin : In patients taking erythromycin, a dose of LONDALOP 1 mg once daily should not be exceeded.
Use with Rifampin : In patients taking rifampin, a dose of LONDALOP 2 mg once daily should not be exceeded |
| Overdose |
There is no known specific treatment in Ihe event of overdose of LONDALOP.
In the event of overdose, the patient should be treated symptomatically and supportive measures instituted as required.
Hemodialysis is unlikely to be of benefit due to high protein binding ratio of LONDALOP. |
| Package |
| -2 x 10 F.C tablets p~~ked in PVC/Aluminum blister inside a cartoon box with a leanet. |
| Storage |
| Store at room temperature between 115 -30)·C. Protect from light, Keep away from children. |