| Composition |
• Sitagliptin/ metformin hydrochloride 50 mg/500 mg tablet
• sitagliptin /metformin hydrochloride 50 mg/1000 mg tablet |
| Pharmacodynamics properties |
| Antihypertensive drugs for oral blood sugar. |
| Properties |
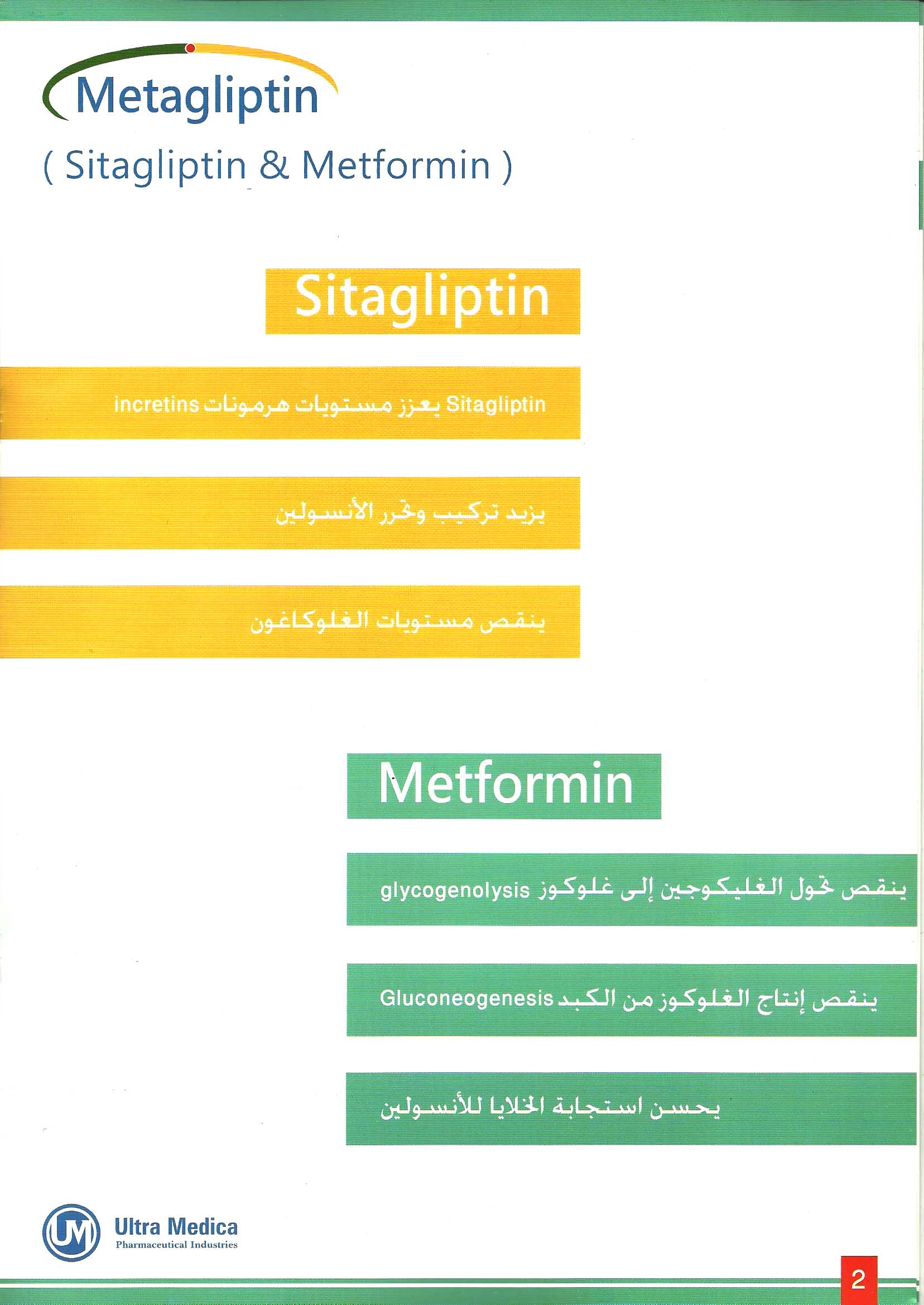
Janumet combines two antihyperglycemic agents with complementary mechanisms of action to improve glycemic control in patients with type 2 diabetes: sitagliptin, a dipeptidyl peptidase-4 (DPP-4) inhibitor, and metformin hydrochloride, a member of the biguanide class.
Sitagliptin
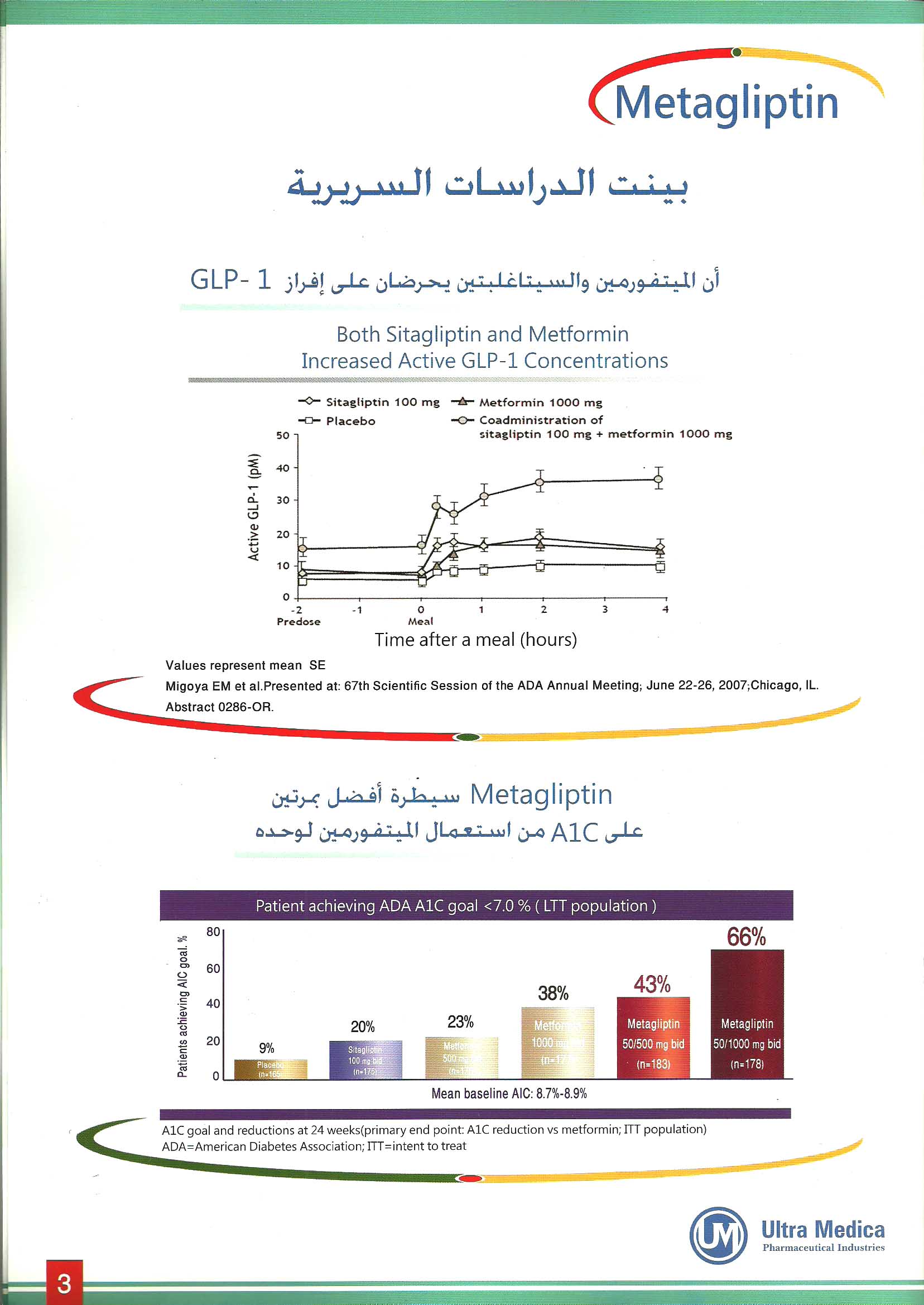
Sitagliptin is a DPP-4 inhibitor, which is believed to exert its actions in patients with type 2 diabetes by slowing the inactivation of incretin hormones. Concentrations of the active intact hormones are increased by sitagliptin, thereby increasing and prolonging the action of these hormones. Incretin hormones, including glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), are released by the intestine throughout the day, and levels are increased in response to a meal. These hormones are rapidly inactivated by the enzyme DPP-4. The incretins are part of an endogenous system involved in the physiologic regulation of glucose homeostasis. When blood glucose concentrations are normal or elevated, GLP-1 and GIP increase insulin synthesis and release from pancreatic beta cells. GLP-1 also lowers glucagon secretion from pancreatic alpha cells, leading to reduced hepatic glucose production. By increasing and prolonging active incretin levels, sitagliptin increases insulin release and decreases glucagon levels in the circulation. Sitagliptin demonstrates selectivity for DPP-4 and does not inhibit DPP-8 or DPP-9 activity in vitro at concentrations approximating those from therapeutic doses.
Metformin hydrochloride
Metformin is an antihyperglycemic agent which improves glucose tolerance in patients with type 2 diabetes, lowering both basal and postprandial plasma glucose. Its pharmacologic mechanisms of action are different from other classes of oral antihyperglycemic agents. Metformin decreases hepatic glucose production, decreases intestinal absorption of glucose, and improves insulin sensitivity by increasing peripheral glucose uptake and utilization. Unlike sulfonylureas, metformin does not produce hypoglycemia in either patients with type 2 diabetes or normal subjects (except in special circumstances [see Warnings and Precautions (5.8)]) and does not cause hyperinsulinemia. With metformin therapy, insulin secretion remains unchanged while fasting insulin levels and day-long plasma insulin response may actually decrease. |
| Therapeutic indications |
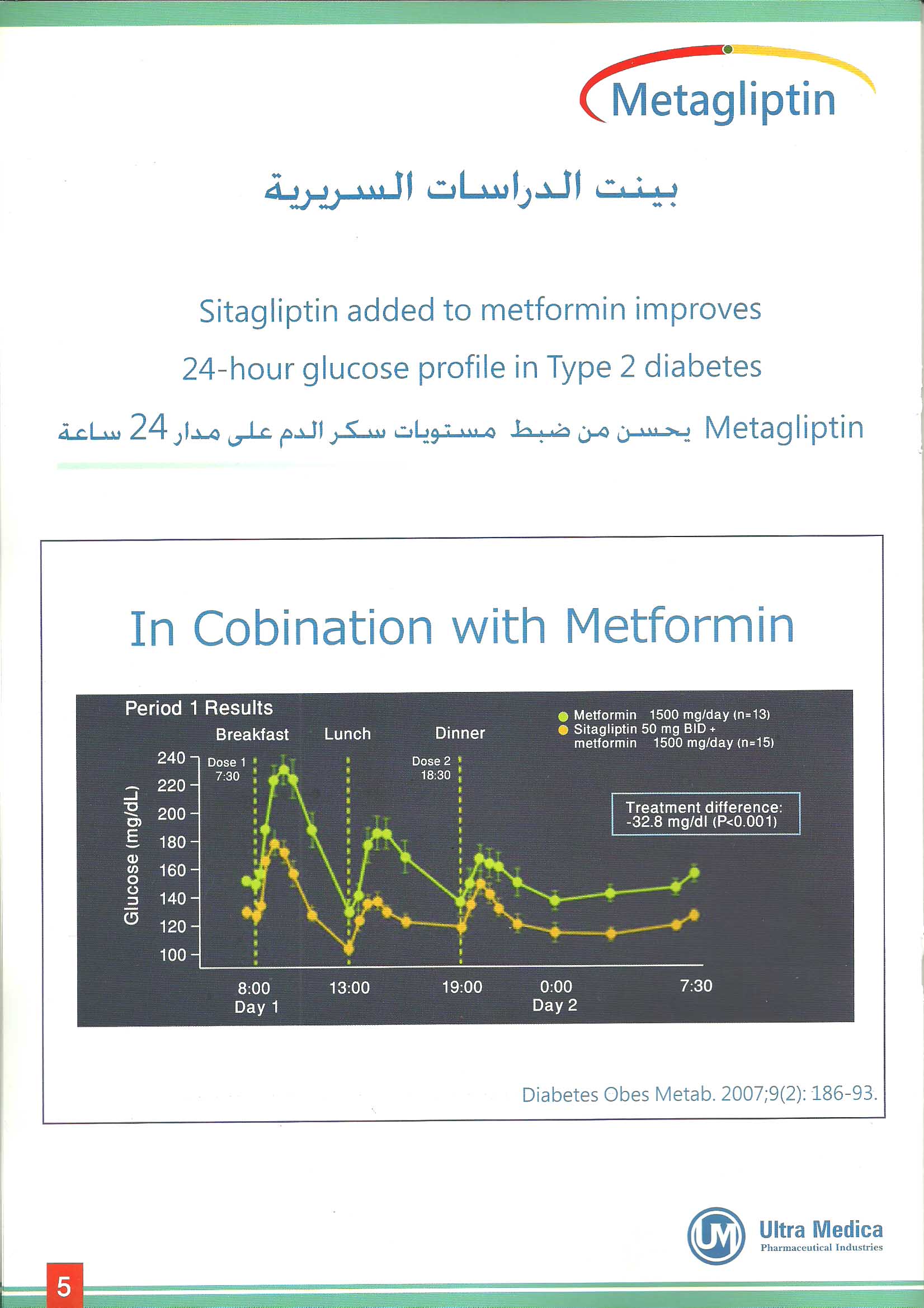
Metagliptin is indicated as an adjunct to diet and exercise to improve glycemic control in adult patients with type 2 diabetes mellitus who are not adequately controlled on metformin or sitagliptin alone or in patients already being treated with the combination of sitagliptin and metformin.
Important Limitations of Use: Metagliptin should not be used in patients with type 1 diabetes or for the treatment of diabetic ketoacidosis. |
| Side effect |
The most common adverse experience in sitagliptin monotherapy reported regardless of investigator assessment of causality in ≥5% of patients and more commonly than in patients given placebo was nasopharyngitis. In most but not all studies, a small increase in white blood cell count.
The most common (>5%) established adverse reactions due to initiation of metformin therapy are diarrhea, nausea/vomiting, flatulence, abdominal discomfort, indigestion, asthenia, and headache. |
| Contraindication |
Metagliptin is contraindicated in patients with:
• Renal disease or renal dysfunction, e.g., as suggested by serum creatinine levels ≥1.5 mg/dL.
• Acute or chronic metabolic acidosis, including diabetic ketoacidosis, with or without coma.
• Metagliptin should be temporarily discontinued in patients undergoing radiologic studies involving intravascular administration of iodinated contrast materials, because use of such products may result in acute alteration of renal function |
| Warnings and precautions |
Lactic acidosis is a rare, but serious complication that can occur due to metformin
accumulation. The risk increases with conditions such as sepsis, dehydration, excess alcohol
intake, hepatic insufficiency, renal impairment, and acute congestive heart failure.
The onset is often subtle, accompanied only by nonspecific symptoms such as malaise,
myalgias, respiratory distress, increasing somnolence, and nonspecific abdominal distress.
Laboratory abnormalities include low pH, increased anion gap and elevated blood lactate.
If acidosis is suspected, JANUMET1 should be discontinued and the patient hospitalized
immediately.
• Lactic acidosis is a rare, but serious, metabolic complication that can occur due to metformin
• Janumet should generally be avoided in patients with evidence of hepatic disease.
• Metformin and sitagliptin are known to be substantially excreted by the kidney. Before initiation of therapy with Janumet and at least annually thereafter, renal function should be assessed and verified as normal.
• Metformin decreases to subnormal levels of previously normal serum Vitamin B12 levels, without clinical manifestations, was observed in approximately 7% of patients. Measurement of hematologic parameters on an annual basis is advised in patients on Janumet. Certain individuals (those with inadequate Vitamin B12 or calcium intake or absorption) appear to be predisposed to developing subnormal Vitamin B12 levels. In these patients, routine serum Vitamin B12 measurements at two- to three-year intervals may be useful.
• Alcohol is known to potentiate the effect of metformin on lactate metabolism. Patients, therefore, should be warned against excessive alcohol intake, acute or chronic, while receiving Janumet.
• Use of Janumet should be temporarily suspended for any surgical procedure (except minor procedures not associated with restricted intake of food and fluids) and should not be restarted until the patient's oral intake has resumed and renal function has been evaluated as normal. |
| Pregnancy and lactation |
Pregnancy Category B: There are no adequate and well-controlled studies in pregnant women with Janumet or its individual components; therefore, the safety of Janumet in pregnant women is not known. Janumet should be used during pregnancy only if clearly needed.
Nursing Mothers: Because many drugs are excreted in human milk, caution should be exercised when Janumet is administered to a nursing woman. |
| Drug interactions |
Cationic drugs (e.g., amiloride, digoxin, morphine, procainamide, quinidine, quinine, ranitidine, triamterene, trimethoprim, or vancomycin) that are eliminated by renal tubular secretion theoretically have the potential for interaction with metformin by competing for common renal tubular transport systems. Careful patient monitoring and dose adjustment of Janumet and/or the interfering drug is recommended in patients who are taking cationic medications that are excreted via the proximal renal tubular secretory system.
Such interaction between metformin and oral cimetidine has been observed in normal healthy volunteers, with a 40% increase in plasma and whole blood metformin AUC.
Digoxin, as a cationic drug, has the potential to compete with metformin for common renal tubular transport systems, thus affecting the serum concentrations of either digoxin, metformin or both. Patients receiving digoxin should be monitored appropriately.
Nifedipine appears to enhance the absorption of metformin. Metformin had minimal effects on nifedipine. |
| DOSAGE & ADMINISTRATION |
| The starting dose of Metagliptin should be based on the patient’s current regimen. Metagliptin should be given twice daily with meals. The usual starting dose of Metagliptin should be twice daily. For patients taking metformin 850 mg twice daily, the recommended starting dose of Metagliptin is 50 mg sitagliptin/1000 mg metformin hydrochloride twice daily. |
| Overdose |
Sitagliptin: During controlled clinical trials in healthy subjects, single doses of up to 800 mg sitagliptin were administered. Maximal mean increases in QTc of 8.0 msec were observed in one study at a dose of 800 mg sitagliptin, a mean effect that is not considered clinically important. In the event of an overdose, it is reasonable to employ the usual supportive measures, e.g., remove unabsorbed material from the gastrointestinal tract, employ clinical monitoring (including obtaining an electrocardiogram). In clinical studies, Sitagliptin approximately 13.5% of the dose was removed over a 3- to 4-hour hemodialysis session.
Metformin hydrochloride: Overdose of metformin hydrochloride has occurred, including ingestion of amounts greater than 50 grams. Hypoglycemia was reported in approximately 10% of cases, but no causal association with metformin hydrochloride has been established. Lactic acidosis has been reported in approximately 32% of metformin overdose cases. Hemodialysis may be useful for removal of accumulated drug from patients in whom metformin overdosage is suspected. |
| Package |
Metagliptin 500: Carton box of 20 Coated tablets, blister packed.
Metagliptin 1000: Carton box of 20 Coated tablets, blister packed.
|
| Storage |
Store in a dry place up to 25ºC
|